Often, a disc herniation is regarded to be small based on its measurements. In reality, measure is not what makes a disc herniation. Rather, size has to do with whether or not the herniation is pressing on the nervous structures of the spine. A small herniation is one that does not contact or impress upon the thecal sac (spinal nerve sac) or any of the nerves that travel through the spinal canal. Small herniations are usually “contained,” meaning that the tear in the annulus (lining of the disc) is not full thickness. In these contained herniations the annular tear usually starts on the inside and extends part way to the periphery of the annulus. Usually, there is a small to moderate amount of disc material contained within this tear.
Large herniations, on the other hand, are those that do press on nervous structures. The tear is usually near or full thickness and there is a moderate to large amount of disc material passing through the tear.
Measuring a herniation’s size is often not helpful. A particular herniation may not be considered large in a 200-pound over 6-foot male. The same size herniation may be quite large in a petite 90-pound female. In the latter case the spinal canal is so small that the same size herniation may compress nervous structures.
Small herniations vs disc bulges
Small herniations are quite common, much more so than large ones. Unfortunately, they are often miss-diagnosed as bulges. Second opinion consultations from a qualified specialist may be helpful. If the protrusion occupies less than 25% of the disc circumference, it is a small contained disc protrusion (figure 1),
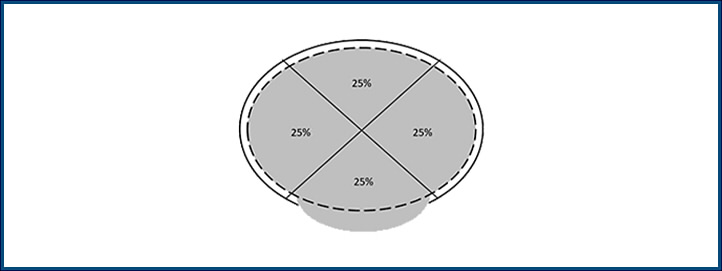
Figure 1
When disc material (shaded) extends beyond its normal margin (dashed line) and the normal vertebra margin (solid line), but involves less than 25% of the disc circumference a herniation is present. This type of herniation is called a protrusion.
not a bulge (figure 2).
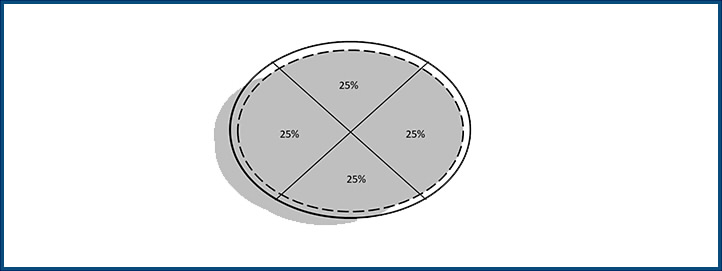
Figure 2
When the disc material protrudes beyond greater than 25% of the disc circumference experts call it a disc bulge.
Disc inflammation
Outdated medical knowledge, still firmly espoused by defense experts and attorneys, has it that a herniation or protrusion must be large enough to be pushing on nerves to cause pain. This has been scientifically refuted since the mid 1990’s. We now know that a small disc protrusion can set in motion a biochemical cascade in the spine. A disc protrusion results in the expression of small inflammatory protein molecules, called cytokines. These molecules include interleukins, tumor necrosis factor, interferon and colony stimulating factors, to name a few. These molecules signal cells associated with inflammation to migrate to the disc injury site. This results in an ingrowth of microscopic blood vessels and even new nerves. Some cytokines even stimulate the expression of other molecules, like prostaglandins, that maintain the vicious cycle of inflammation. Prostaglandins are very important inflammatory molecules that are inhibited by drugs like aspirin and ibuprofen.
The inflammatory cascade begins with a tear in the disc and ends in a painful and inflamed disc. With time, the disc becomes even more painful because of the ingrowth of new nerve endings, thanks to the cytokines and inflammation. Often, the inflammation will extend beyond the disc to involve the nerves, explaining why a small protrusion can cause radiculopathy, or nerve pain. The inflammation may cause the nerves to become swollen, inflamed and even scarred.
Diagnosis and treatment of small disc herniations
When a small herniation is suspected in a patient with significant pain, additional steps are undertaken. An epidural injection may break the inflammatory cascade. If unsuccessful, surgery may be necessary.
With small herniations it is important to avoid a destructive procedure like a fusion. In a small herniation only a limited portion of the disc is abnormal. Demolishing the entire disc to perform a fusion is overkill. Discectomy, a procedure where only the disc interposed between the torn annulus is removed, usually yields good results.
Conclusion
A small herniation is worth investigating if it is causing significant pain, disability and impairment. The MRI must be read properly and must not be confused with a bulge. There is a preponderance of scientific evidence that points to the presence of inflammation as a source of pain in protrusions. Epidurals are a first line treatment. If conservative care is ineffective conservative forms of surgery are good options.
Horace Couchman, MD
The views expressed are the personal views of the author and do not represent the views of The Brain, Spine and Joint Group, its managers, affiliates, partners, employees or its clients. Furthermore, the information provided by the author is not intended to be expert or legal advice.
The content of this newsletter is confidential. It is strictly forbidden to copy, forward, reveal the content of or share any part of this newsletter content with any third party, without a written consent of The Brain, Spine and Joint Group. If you received this newsletter, or a link to it, by mistake, please message